The Science Behind MIPD: No Two Patients Are the Same
For decades, drug dosing has followed a simple formula: weight times a fixed milligrams-per-kilogram number. It works well enough as a starting point. But for drugs with narrow therapeutic windows, "good enough" isn't really good enough.
Standard dosing treats every patient as an average. MIPD uses patient data, measured in real time, to individualize drug exposure for the person in front of you.
Clinical practice is already moving in this direction. The 2020 joint consensus guidelines from ASHP, IDSA, PIDS, and SIDP recommend AUC-guided vancomycin monitoring using Bayesian software as the preferred approach, reflecting a broader shift toward model-informed methods at the point of care. MIPD is the framework that makes this possible across drug classes and patient populations.
The approach is most established for drugs with narrow therapeutic windows, including vancomycin, aminoglycosides, busulfan, and tacrolimus, but the underlying framework can apply to any drug where individual PK variability would meaningfully affect outcomes.
The Prior: What a Population Model Actually Knows
Give 1,000 patients the same weight-based dose. You'll get 1,000 different exposure profiles. A population pharmacokinetic model doesn't ignore that variability — it encodes it, giving every dosing decision a realistic starting point before the first level is drawn.
MIPD applies whether or not a drug level has been drawn. Population PK models can generate optimized dose recommendations from patient characteristics alone, before any samples are collected. When levels are available, Bayesian estimation incorporates them to refine the individual estimate further. The two approaches work on a continuum: population models set the prior, measured data sharpens it.
The case for individualization is well-documented. Antifungal therapy is a major determinant of survival in critically ill patients with invasive fungal disease, yet standard dosing left more than 25% of treatment patients below predefined PK/PD targets early in therapy, with target attainment as low as 41.7% for amphotericin B, 57.1% for voriconazole, 63.2% for posaconazole, and 64.1% for micafungin. Clinical failure, in turn, was a strong independent predictor of 30-day mortality across agents (Roberts et al., 2025). The chain from inadequate dosing to poor outcomes runs through a system that never accounts for the individual patient's pharmacokinetics.
Balancing the Pulls: From Population to Individual
Once a drug level or surrogate biomarker is drawn, there's no reason to keep treating this patient as a population average. Bayesian estimation takes that measurement (from a single point in time) and uses it to pull the population prediction toward this individual's true pharmacokinetic profile.
The model weighs the prior population estimate against the information in the observed sample, and narrows the range of plausible curves. Additional samples narrow it further. The model is no longer working only from population statistics, and instead now incorporates population estimates alongside your individual patient.
A Good Estimate vs. The Right Dose: Where Standard Dosing Can Fall Short
MIPD doesn't rely on any single measurement or any single moment. It integrates the full observed profile (including when samples were drawn, how concentrations have changed over time, and what the population model predicts about this patient's underlying PK) to arrive at a dose that is calibrated to the individual.
Standard equations apply the same math to every patient. The scenarios below show what happens when that assumption breaks — and what individualized dosing sees that a calculator can't.
Dosing That Learns and Adapts: The Evidence for MIPD
Outdated dosing methods made sense when the only alternative was intuition. Today, the data exists to do better. Population models built from real patient outcomes, Bayesian methods that individualize in real time, and software that makes this workflow practical at scale.
The evidence is consistent. Bayesian MIPD has been shown to:
- Reduce AKI events due to vancomycin dosing by a relative 75% (Neely et al., 2018)
- Shorten hospital stays by an average of 2 days (Hall et al., 2024)
- Decrease time per intervention and nearly double the proportion of usable lab samples (Alsowaida et al., 2022)
- Reduce costs over trough-based approaches by more than $2,000 per patient, and over 2-level AUC methods by more than $800 per patient (Lee et al., 2020)
MIPD doesn't replace clinical judgment. It gives clinicians better information to act on — at the moment it matters, and for the patient in front of them.
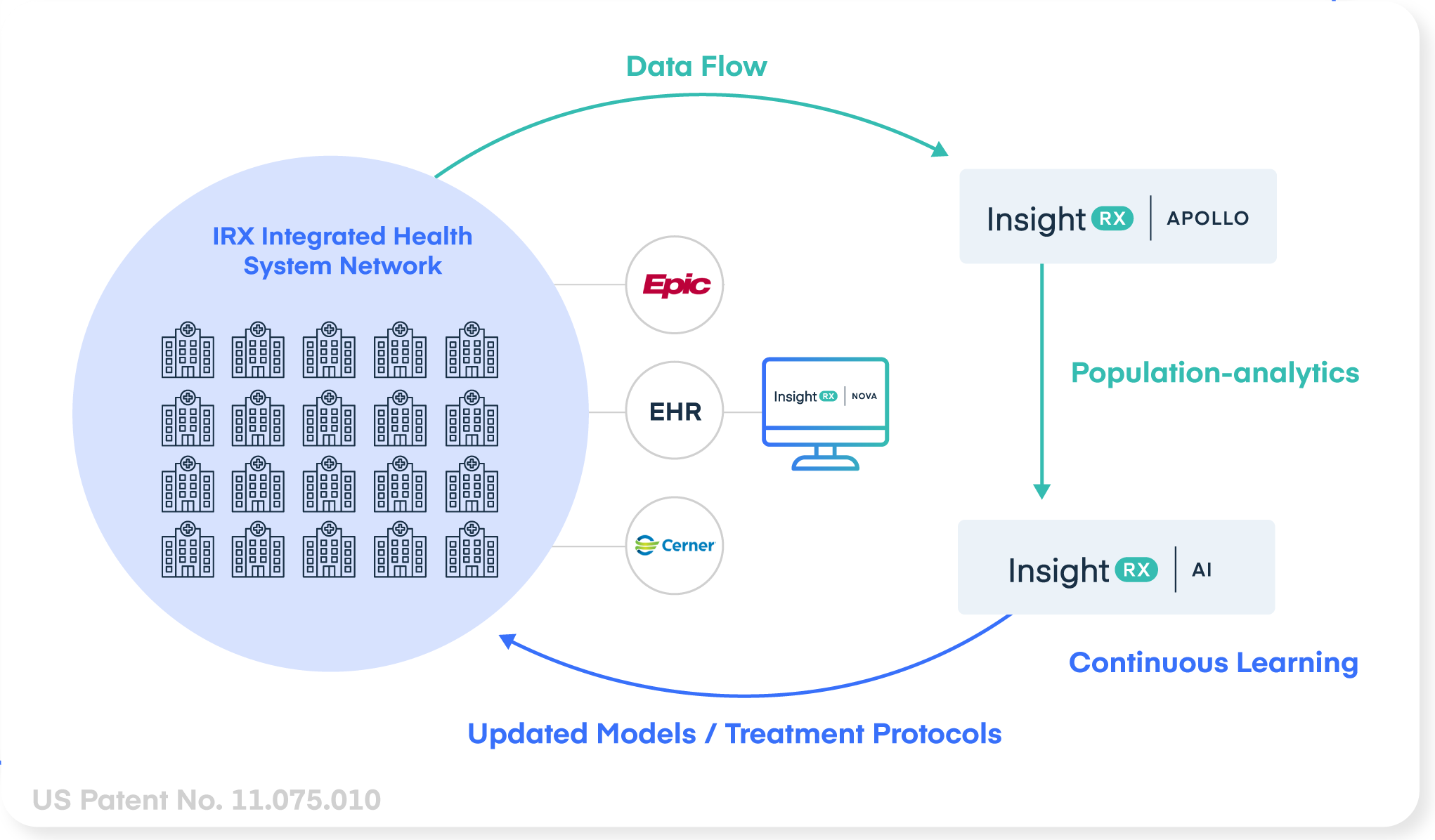
InsightRX MIPD
Powered by science and innovation
InsightRX Nova, Apollo, and Continuous Learning work together as an end-to-end solution platform, delivering individualized dosing that adapts to every patient and improves over time:
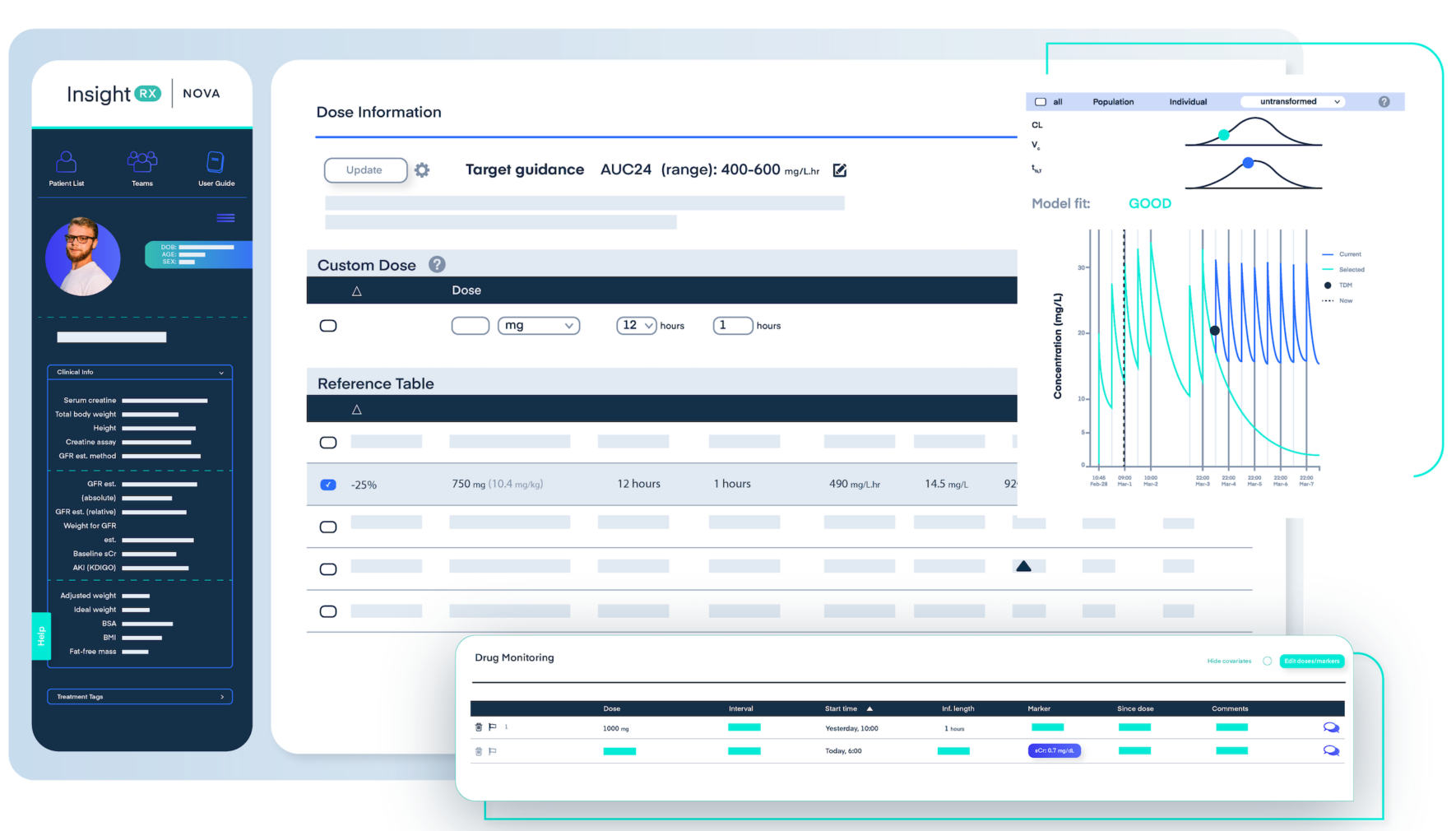
InsightRX Nova

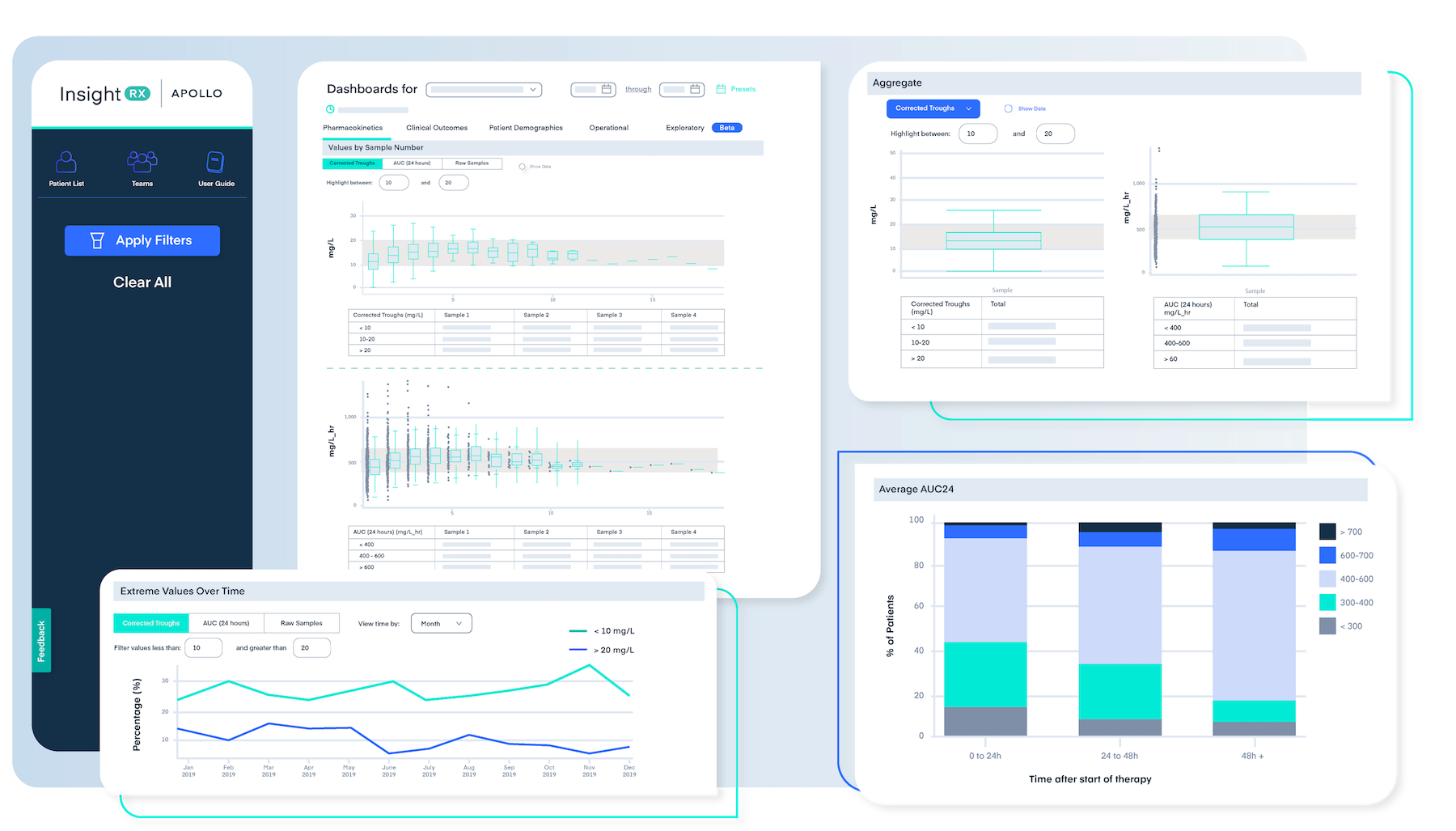
InsightRX Apollo

Continuous Learning